- Research
- Open access
- Published:
Effect of ultrasound parameters of benign thyroid nodules on radiofrequency ablation efficacy
BMC Medical Imaging volume 23, Article number: 85 (2023)
Abstract
Background and aim
Ultrasound-guided radiofrequency ablation (RFA) is a minimally invasive therapy for thyroid nodules (TNs). Understanding the determinants of RFA efficacy can improve treatment and prognosis. This study aims to investigate the relationship between ultrasound parameters of benign TNs and the efficacy of RFA.
Methods
A pretest–posttest interventional study was conducted in 2021 on 250 randomly sampled patients with benign TNs, receiving RFA. For this purpose, the volume reduction (VR) and the VR ratio (VRR) of the nodules were measured at the 1-, 3-, 6-, and 12-month follow-up periods after the RFA completion. The technical success rate (TSR) of this procedure was then categorized into four states, including low (VRR < 25%), moderate (VRR = 25–49%), high (VRR = 50–74%), and very high (VRR ≥ 75). Ordered logistic regression (OLR) was further utilized to investigate the effect of the ultrasound parameters of TNs on the TSR. The analyses were notably performed using Stata 14.2.
Results
The VRR at the 1-, 3-, 6-, and 12-month follow-up periods were 38.7%, 53.6%, 59.3%, and 59.9%, respectively. The mean VR was also statistically significant at all follow-ups (p < 0.001). At the 1-, 3-, and 6-month follow-up periods, the VR of over 50% was observed in 28.2%, 52.1%, and 65.2% of the nodules, respectively. The odds ratios (ORs) of the RFA success were found to be 4.3 times higher for the nodules in the left lobe compared to the right lobe (OR: 4.31, p = 0.002), 6.3 times greater for isoechoic nodules compared to hyperechoic nodules (OR: 6.39, p < 0.001), 6.2 times higher for hyper-vascular nodules compared to hypo-vascular nodules (OR: 6.25, p = 0.005), and 2.3 times greater for mixed nodules compared to solid ones (OR: 2.37, p = 0.049).
Conclusion
The ultrasound parameters of TNs had a statistically significant effect on the efficacy of RFA. Small-sized, isoechoic, and hyper-vascular nodules, as well as those with mixed tissue, were observed to respond better to RFA, leading to a better prognosis in terms of VR after treatment.
Introduction
Thyroid nodules (TNs) are among the common diseases of the endocrine system [1]. According to the autopsy and ultrasound reports, roughly 40–50% of the world’s general population suffer from the abnormal overgrowths of tissue in the thyroid gland [2]. Such nodules can be identified in 4–7% of the general population through physical examinations, or via palpation in 1.5% and 6% of men and women, respectively [3, 4]. Autopsy and ultrasound reports also suggest that approximately 30–70% of TNs form in middle-aged people (namely, 50 years of age on average) and that they are more common in Asian populations [4].
Overgrown TNs tend to put much pressure on the surrounding tissue, causing discomfort and sensation of a foreign body in the throat, swallowing difficulties, hoarseness, shortness of breath, and external symptoms. If left untreated, these nodules may result in life-threatening conditions, such as acute respiratory arrest (ARA) [5]. Even if TNs are diagnosed as benign during a biopsy, there is a 6% probability to be malignant in a post-operative autopsy, as evidenced in previous research [6]. Therefore, it has been recommended to treat symptomatic benign TNs actively, as if they were potentially malignant, in order to prevent any potential life-threatening complications [7].
Considering the risks associated with surgery (even simple lobectomy) on TNs, including laryngeal paralysis, scarring, infection, compressive hematoma, hypocalcemia, and lifelong hormone replacement therapy (HRT) [8] for the benign cases, it is better to practice less invasive and expensive treatment methods. Radiofrequency ablation (RFA) has been accordingly recommended as the first-line therapy for some cases [9]. Despite the availability of guidelines for managing TNs, surgery is still excessively used as the first-choice treatment, which has become a challenge [10]. Along with the latest evidence in France, nearly 10,000 unnecessary thyroidectomies are done each year in patients with the most-likely benign nodules [11]. In one study, more than half of the operated TNs were thus found to be benign after surgery, indicating a trend of over-surgery on them [12].
Ultrasound-guided RFA is known as a minimally invasive non-surgical therapy that was first employed for the treatment of benign and advanced malignant liver tumors [13]. Considering the advantages of this procedure in terms of safety, efficacy, lack of incision and scarring, and absence of hormone therapy after completion, it is a viable choice to treat benign TNs and even hard-to-operate malignant ones [14, 15]. Given the relatively short history of the application of RFA in the treatment of TNs, many questions still remain regarding the determinants of its efficacy [16].
To improve RFA efficacy and minimize its side effects, it is crucial to shed light on the factors that may affect how well this procedure can deliver the planned results. As evidenced in the related literature, RFA tends to reduce the volume of TNs and alleviate their symptoms over time [17]. However, to the best of the authors’ knowledge, the present study is the first attempt to investigate the effect of ultrasound parameters of TNs (including tissue condition, echogenicity, vascularity, etc.) on its efficacy. The efficacy of RFA was examined in this study to determine whether and how much it was influenced by the ultrasound parameters of TNs.
Methods
This interventional study was conducted in 2021 on a population of randomly selected Iranian patients with benign TNs who received RFA. Using the sample size formula for studies with a pretest–posttest design with a 5% error and 95% confidence interval (CI) for an expected effect size of 37% based on previous studies [5], the minimum sample size was determined to be 96 cases. However, it was decided to recruit a sample size of 250 to improve the accuracy of the findings and account for the possibility of dropouts. The random selection process was conducted among the pool of eligible patients referred by an Endocrinology specialist, and each eligible patient had an equal chance of being chosen. The selection was not based on any specific characteristics such as patient age, sex, or nodule size, but rather on the patient’s eligibility for RFA treatment, which was determined by the Endocrinology specialist based on the patient’s clinical condition and the characteristics of the thyroid nodules. Out of the 250 patients, 66 cases were excluded because they did not return in time for the 1-, 3-, 6-, and 12-month follow-up periods. Therefore, data from 184 patients were ultimately collected and analyzed. The participation and dropout rates were also equal to 74% and 26%, respectively.
The inclusion criteria for this study were as follows: age of at least 18 years old, diagnosis of benign TNs confirmed by two-time fine needle aspiration (FNA) biopsies, euthyroidism, normal profile of thyroid hormones in blood tests, and informed consent. Patients for whom TN treatment was not indicated, such as those who did not experience swallowing difficulties, shortness of breath, hoarseness, sensation of a foreign body in the throat, or dissatisfaction with their appearance, were excluded from the study. Additionally, patients with hypothyroidism and hyperthyroidism were also excluded. The data collection was performed in three stages:
-
Stage 1: The demographic characteristics of the patients (i.e., age and gender) and the ultrasound parameters of the TNs (i.e., nodule size in diameter, tissue condition, echogenicity, vascularity, and location) were collected from the diagnostic imaging and pathological reports, along with the ultrasound results. The nodule volume was automatically calculated in cm^3 (equivalent to milliliters, ml) by the ultrasound device using the ellipsoid formula based on the measurements of the nodule’s three dimensions (length, width, and height). These measurements were taken by experienced radiologists using standardized protocols to ensure consistency and accuracy. Moreover, the measurements were obtained in multiple planes to ensure accuracy and minimize error. The before-after treatment images are presented in the Fig. 1.
Fig. 1 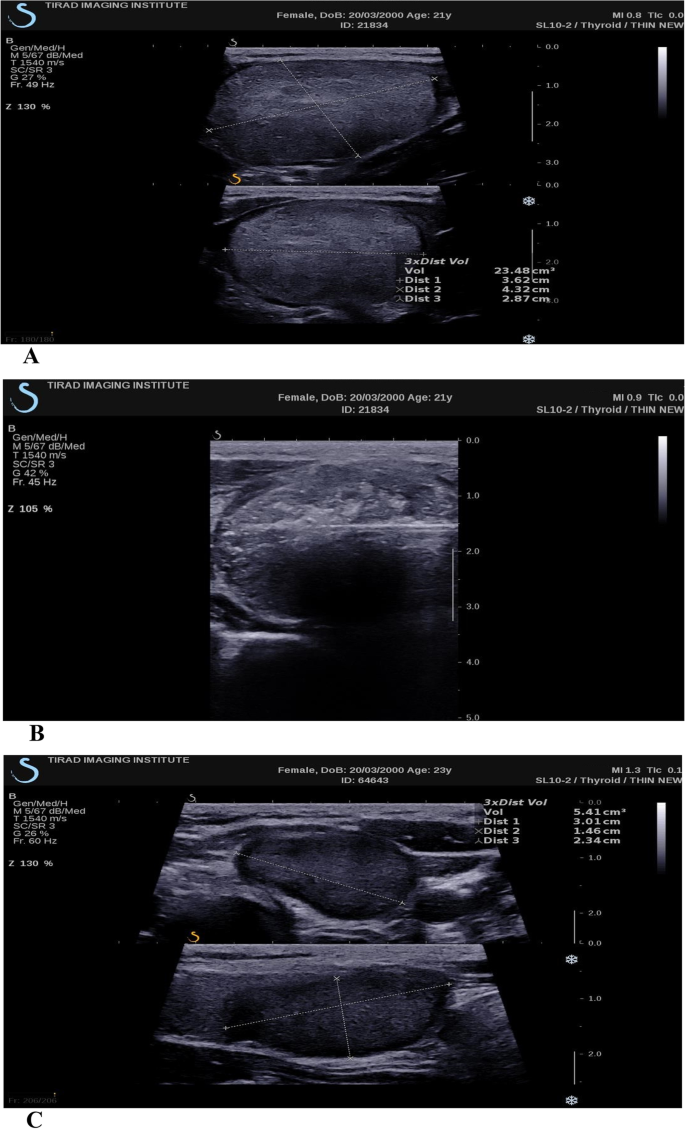
A Thyroid nodule size before RFA treatment, B RFA procedure on thyroid nodule, and C Post-RFA, 12-month follow-up of thyroid nodule
-
Stage 2: The patients underwent RFA, wherein an RFA System was used to emit radio waves proportional to the nodule size according to the protocol [18], causing the destruction of nodule cells through friction and heat transfer. The data collected at this stage included the date and description of the RFA procedure. It is worth noting that an interventional radiologist with 7 years of experience performed the RFA treatment and was assisted by one radiology resident who provided support during the treatment under the guidance of the experienced radiologist.
-
Stage 3: The change in nodule size after RFA was measured by ultrasound during the 1-, 3-, 6-, and 12-month follow-up periods. To minimize the impact of the measurement error on the findings, all RFA procedures and the nodule size pre- and post-measurements were completed by the same interventional radiologist, using the same machines and the same method.

In the descriptive phase of the study, the mean nodule volume reduction (VR) in ml and the VR ratio (VRR) in percentage (%) at the 1-, 3-, 6-, and 12-month follow-ups were calculated. The technical success situation (TSS) and the technical success rate (TSR) were further measured and reported as the measures of the RFA efficacy. Following the approach taken in previous studies [19], the TSS was defined as an over 50% reduction in the nodule size. Accordingly, two states were outlined for the TSS, viz., success (over 50% VR) and failure (below 50% VR). Moreover, the TSR was quartered at four states, namely, low (below 25% VR), moderate (25–49% VR), high (50–74% VR), and very high (75–100% VR).
In the analytical phase of the study, the comparison of the means was used to examine the RFA efficacy by checking whether the nodule size had significantly changed after the procedure. Since the Shapiro–Wilk test outcomes rejected the normality of the data, the non-parametric Wilcoxon signed-rank test was utilized to compare the mean nodule sizes before and after RFA. Finally, the ordered logistic regression (OLR) was employed to determine the effect of the ultrasound parameters of TNs on the TSR. As well, the TSR was introduced into the regression model as a qualitative ordinal variable (with low, moderate, high, and very high success) and the effect of the ultrasound parameters on this variable was investigated. All data analyses were performed using Stata 14.2.
This study was conducted in compliance with all the principles of professional and scientific ethics along with the full observance of the confidentiality of patient information. Informed consent was further obtained from all participants. All experimental protocols were additionally approved by the Iran National Committee for Ethics in Biomedical Research with the code no. IR.AJAUMS.REC.1400.071, ensuring adherence to the guidelines set forth by this committee. Furthermore, the study followed relevant international clinical practice guidelines for radiofrequency ablation of benign thyroid nodules, to ensure the ethical conduct of the research and protection of human subjects.
Results
The mean VR (in ml) and VRR (in %) at the 1-, 3-, 6-, and 12-month follow-up periods are presented in Table 1. One month after RFA, a decrease in the size of all nodules was observed, with a mean VR of 17.6 ml (38.7% VRR). Additionally, the mean VR in the 3-, 6-, and 12-month follow-ups was 24.5 ml (53.6% VRR), 27.8 ml (59.3% VRR), and 27.8 ml (59.9% VRR), respectively. The median of VRR was 36.1%, 54.2%, 61%, and 61.3% at 1, 3, 6, and 12 months after RFA, respectively. Regarding the marginal changes in VRR (i.e., changes in the current follow-up VR compared with the previous one), the results indicated that the greatest VRR occurred during the first month (with an average of 38%), and the VRR decreased over time. Specifically, the nodule volume decreased by only 14% on average from the first to the third month and by 5% on average from the third to the sixth month. After the sixth month, the volume change was not significant, and the marginal change in VRR for the 12-month follow-up period (compared with the 6-month follow-up) was below 1% (0.53%).
The mean sizes of TNs before and after the RFA procedure are compared in Table 2. In this line, the TN size reductions at all follow-ups were found to be statistically significant (p < 0.001).
The TSS and TSR results are reported in Table 3 and plotted in Fig. 2. Based on the findings in Table 3, it was observed that the TSS of RFA (VRR > 50%) improved over time, increasing from 28.2% at the 1-month follow-up to 52.1% at the 3-month period, 65.2% at the 6-month follow-up, and finally settling at 64% one year after the RFA completion.

TSR of RFA at 1- to 12-month follow-ups
The TSR results presented in Fig. 2 illustrate that during the first month after RFA, low success was observed for 25% of the nodules, but this value decreased to 2% at the 6-month follow-up. Additionally, RFA was observed to be highly successful (VRR > 75%) for only 5% of the nodules at the 1-month follow-up, but this value increased to 21% at the 12-month follow-up (Fig. 2).
The OLR analysis in Table 4 examined the impact of ultrasound parameters of TNs on the TSR, and the results suggest that, holding other factors constant:
-
RFA is three times more likely to succeed on small-sized nodules than large-sized nodules (OR: 3.02, p = 0.004).
-
RFA is two times more likely to succeed on left-lobe nodules than right-lobe nodules (OR: 2.03, p = 0.031).
-
RFA is 5.3 times more likely to succeed on hypoechoic nodules than hyperechoic nodules (OR: 5.36, p = 0.004).
-
RFA is 3.2 times more likely to succeed on isoechoic nodules than hyperechoic nodules (OR: 3.26, p = 0.003).
-
RFA is 4.1 times more likely to succeed on hyper-vascular nodules than hypo-vascular nodules (OR: 4.14, p = 0.002).
-
RFA is 6.6 times more likely to succeed on mixed nodules than cystic nodules (OR: 6.66, p = 0.004).
-
RFA is 2.4 times more likely to succeed on mixed nodules than solid nodules (OR: 2.45, p = 0.006).
The results also demonstrated a statistically significant relationship between gender and the RFA success. Assuming that other factors were constant, RFA was 2.8 times more likely to be successful in men than in women (OR: 2.83, p = 0.008).
Discussion
In this study, the mean and median of the nodule VRR one year after RFA completion were 59.9% and 61.3%, respectively. The TSS of RFA at the 12-month follow-up was also 64%, implying that 12 months after this procedure, 64% of the nodules had more than 50% VR. The first report on the clinical use of RFA on benign TNs in Iran was published by Ebrahiminik et al. [20] in the Iranian Journal of Radiology in 2017. They successfully treated 50 patients with 63 solid or cystic nodules with RFA, achieving 40–67% VRR at 1- and 3-month follow-up periods. In a similar investigation in 2021 by Deandrea et al. [18] on 115 Italian patients with benign TNs, the median VRR at the 12-month follow-up was 64% and the TSS was 75%. It was also described that one year after RFA, many patients, even those with below 50% VRR, no longer had compressive and cosmetic symptoms.
In the present study, the mean nodule VRR in the 1-, 3-, 6-, and 12-month follow-ups after RFA was 38.7%, 53.6%, 59.3%, and 59.9%, respectively, and their corresponding medians were 36.1%, 54.2%, 61%, and 61.3%, in that order. In Bisceglia et al. [21], examining 119 patients with benign TNs with a 48-month follow-up from 2014 to 2018, the mean VRR was 47.1%, 55.3%, 61.2%, and 67.7% in the 1-, 3-, 6-, and 12-month follow-up periods, respectively. A significant progressive improvement was further reported in VRR in the first two years after RFA up to the 24-month follow-up. In the present study, however, the greatest VR took place at the 1-month follow-up and its ratio dwindled over time, ultimately dropping to 0.53% at the 12-month period compared with the 6-month one. In this respect, Kuo et al. [22], investigating 109 nodules in 93 patients, found that the mean VRR was 55.9% six months after RFA. AAs well, Nguyen et al. [23], in a study on 78 benign TNs correspondingly reported the mean VRR of 41.4% and 64.7% and the TSR (VRR > 50%) of 30.8% and 84.6% at the 1- and 3-month follow-ups, respectively.
The results of the present study additionally established that the location of TNs could influence the success of the RFA procedure. More specifically, RFA was 2 times more likely to be successful on the left-lobe nodules than the right-lobe ones (OR: 2.03, p = 0.031). In Kuo et al. [22], reflecting on 102 nodules in 93 patients, VRR was further higher in the left-lobe nodules than the right-lobe ones, but this difference was not statistically significant. Similarly, Lee et al. [7] reported lower success (VRR > 50%) in the right-lobe nodules than the left-lobe ones, but there was no statistically significant difference in this respect (OR: 0.820, p = 0.557). The uneven efficacy of RFA in the left and right lobes could be thus related to the dissimilarities of the lobes in terms of anatomy and also the interventionist’s left- or right-handedness that need to be further examined in future studies.
Besides, the study results demonstrated a significant relationship between the RFA success and the echogenicity of TNs. Specifically, RFA was 5.3 and 3.2 times more likely to be successful on the hypoechoic and isoechoic nodules than the hyperechoic ones (OR: 5.36, p = 0.004; OR: 3.26, p = 0.003), which was consistent with the findings reported by Kuo et al. [24], suggesting a significant negative correlation between echogenicity and VRR in the solid nodules, in the sense that the success rate of RFA diminished as the nodule echogenicity elevated.
In this study, the RFA success was also found to be influenced by the vascularity of TNs. In particular, RFA was 4.1 times more likely to be successful on the hyper-vascular nodules than the hypo-vascular ones (OR: 4.14, p = 0.002). In the recent study by Deandrea et al. [18] on 337 patients in Italy, a significant relationship was similarly observed between the vascularity of TNs and the success of RFA. As well, the hyper-vascular TNs (i.e., those with intense peripheral and intranodal patterns) experienced a greater VR than the hypo-vascular and iso-vascular ones. Besides, a 71% reduction was reported in the hyper-vascular nodules as compared with the values of 68% in the hyper-vascular nodules and 67% in the iso-vascular ones; a difference that was statistically significant (p < 0.03). The reason for the discrepancy in the effectiveness of therapy for the hyper-vascular nodules could be thus explained by the creation of more coagulative necrosis in the hyper-vascular TNs after RFA and the resulting cell death, which could produce more VR in the nodules. In contrast to these findings, Kim et al. [25] in a study in 2006 on 35 nodules reported that vascularity had no significant impact on treatment response (p < 0.05).
The results of the present study confirmed that the RFA success was significantly correlated with the tissue condition of TNs, in the sense that RFA was 6.6 and 2.4 times more likely to be successful on the mixed nodules than the cystic and solid ones, respectively (OR: 6.66, p = 0.004; OR: 2.45, p = 0.006). This relationship could be thus attributed to the lower cellularity of the mixed nodules. The article published in 2006 by Kim et al. [25], as the first attempt on the clinical use of RFA to treat TNs, also reported that the mixed nodules responded significantly better than the solid ones (p < 0.05). Bisceglia et al. [21], examining benign TNs with a long-term follow-up from 2014 to 2018, further observed a significant positive relationship between treatment success (VRR ≥ 75%) and the presence of macrocystic structures (hazard ratio [HR] = 2.48, p = 0.046). As well, Kuo et al. [24] reported a significant relationship between the tissue condition of TNs and the success rate of RFA; namely, the efficacy of this procedure reduced with the higher proportion of the cystic components in nodules. In a study by Aysan et al. in 2016 [2], wherein one-session RFA significantly decreased (p < 0.001) the size of benign TNs from 16.8 ml before this procedure to 4.8 ml at the 3-month follow-up and 2.6 ml at the 6-month follow-up, the size reduction was greater in the cystic nodules than the solid and mixed ones. Deandrea et al. [18], investigating 337 patients in Italy also reported a significant relationship between the tissue condition of TNs and the success rate of RFA. As well, the spongiform TNs experienced a statistically significant (p < 0.01) size reduction (76%) than the solid (66%) and mixed (67%) ones. Likewise, Kuo et al. [22], reflecting on the success factors leading to RFA based on multivariate regression analysis on the data gathered from 109 nodules in 93 patients, showed significantly higher VRR in the cystic nodules than the solid ones (p = 0.04).
In the present study, RFA was 3 times more likely to be successful on the small-sized nodules than the large-sized ones (OR: 3.02, p = 0.004). Similarly, Deandrea et al. [18] reported that the RFA efficacy was negatively correlated with the nodule size, viz., the smaller the nodule, the greater the efficacy, and positively correlated with the amount of energy radiated to the nodule (per ml of the nodule volume). In Bisceglia et al. [21], the large initial nodule size (> 22.4 ml) based on the 4-year follow-up from 2014 to 2018 was found to be a predictor of the failure to achieve a VRR ≥ 75% after RFA (HR = 0.54, p = 0.036). In other words, the nodules with an initial volume of ≤ 22.4 ml responded significantly better to the treatment (p = 0.01). Likewise, Deandrea et al. [18] identified a weak inverse correlation between the initial nodule size and the nodule size reduction ratio (Spearman: -0.23). Feroci et al. [26], recruiting a small sample in Italy, also found that the nodules with an initial size of less than 20 ml had a greater VRR than those larger than 20 ml, and this difference was statistically significant at the 3- and 6-month follow-ups (p < 0.05), but not at the 12-month period (p = 0.167). In this respect, Lee et al. [7] also reported that RFA was 1.8 times more likely to succeed (VRR > 50%) on the nodules smaller than 4 ml than those larger than 4 ml (OR: 1.821, p = 0.032).
The present study correspondingly detected a statistically significant relationship between gender and the RFA success, in the sense that RFA was 2.8 times more likely to be successful in men than women, considering other factors being constant (OR: 2.83, p = 0.008). According to Lee et al. [7], investigating the determinants (VRR > 50%) of the RFA success on 1619 TNs, RFA was 1.2 times more successful in men than women, but this difference was not statistically significant (OR: 1.427, p = 0.430). Nguyen et al. [23], studying 78 benign TNs via multivariate regression analysis showed no statistically significant relationship between VRR and patient age (β: 0.29, p = 0.135) or gender (β: -16.09, p = 0.17). Considering the discrepancy in these findings, future studies are recommended to explore the relationship between the RFA efficacy and the level of sex hormones.
Despite the multitude of studies conducted on the efficacy of RFA in the treatment of benign TNs, little research has thus far investigated the effect of the ultrasound parameters of nodules on the efficacy of this procedure by multivariate regression analysis. In fact, most studies in this field have employed univariate analyses without respecting the effect of the confounding variables. The present study was accordingly the first attempt to perform a multivariate regression analysis with an OLR model to identify the effect of the ultrasound parameters of TNs on the RFA efficacy. Nevertheless, this study had two major limitations. First, almost all (95.6%) nodules examined in this study were non-calcified, which made it statistically impossible to investigate the effect of nodule calcification on the efficacy of RFA. The second limitation was the difficulty of maintaining a larger sample because of the patients’ poor commitment to follow-up schedules (here, the 1-, 3-, 6-, and 12-month follow-up periods), which caused 66 patients to be excluded from the study (of note, the participation rate was 74% and the sample dropout rate was 26%).
Conclusion
The study results suggest that the ultrasound parameters of TNs may have a statistically significant effect on the efficacy of RFA. The small-sized, isoechoic, hyper-vascular nodules, and those with mixed tissue were found to respond better to RFA, resulting in a better prognosis in terms of VR. Therefore, reserving RFA for the appropriate cases and considering alternative treatments for cases where it is unlikely to be effective could improve the efficacy of RFA. The study findings could be helpful in reducing unnecessary and ineffective RFA procedures.
Availability of data and materials
The datasets generated during the study are available from the corresponding author upon reasonable request.
References
Panagiotou G, et al. Association between lifestyle and anthropometric parameters and thyroid nodule features. Endocrine. 2017;56(3):560–7.
Aysan E, et al. Single-session radiofrequency ablation on benign thyroid nodules: a prospective single center study. Langenbecks Arch Surg. 2016;401(3):357–63.
Ben Hamou A, et al. Safety and efficacy of thermal ablation (radiofrequency and laser): should we treat all types of thyroid nodules? Int J Hyperth. 2019;36(1):665–75.
Staničić J, et al. Thyroid nodularity-true epidemic or improved diagnostics. Acta Clin Croat. 2009;48(4):413–7.
Guang Y, et al. Patient satisfaction of radiofrequency ablation for symptomatic benign solid thyroid nodules: our experience for 2-year follow up. BMC Cancer. 2019;19(1):1–8.
Kihara M, et al. Evaluation of cytologically benign solitary thyroid nodules by ultrasonography: a retrospective analysis of 1877 cases. Auris Nasus Larynx. 2013;40(3):308–11.
Lee S, et al. The biopsy-proven benign thyroid nodule: is long-term follow-up necessary? J Am Coll Surg. 2013;217(1):81–8.
Vaiman M, et al. Hypothyroidism following partial thyroidectomy. Otolaryngol Head Neck Surg. 2008;138(1):98–100.
Kim J-H, et al. Summary of the 2017 thyroid radiofrequency ablation guideline and comparison with the 2012 guideline. Ultrasonography. 2019;38(2):125.
Jegerlehner S, et al. Overdiagnosis and overtreatment of thyroid cancer: a population-based temporal trend study. PLoS One. 2017;12(6):e0179387.
Mathonnet M, et al. What is the care pathway of patients who undergo thyroid surgery in France and its potential pitfalls? A national cohort. BMJ Open. 2017;7(4):e013589.
Singh Ospina N, et al. Prognosis of patients with benign thyroid nodules: a population-based study. Endocrine. 2016;54(1):148–55.
Gazelle GS, et al. Tumor ablation with radio-frequency energy. Radiology. 2000;217(3):633–46.
Jeong WK, et al. Radiofrequency ablation of benign thyroid nodules: safety and imaging follow-up in 236 patients. Eur Radiol. 2008;18(6):1244–50.
Deandrea M, et al. US-guided percutaneous radiofrequency thermal ablation for the treatment of solid benign hyperfunctioning or compressive thyroid nodules. Ultrasound Med Biol. 2008;34(5):784–91.
Park HS, et al. Thyroid radiofrequency ablation: updates on innovative devices and techniques. Korean J Radiol. 2017;18(4):615–23.
Durante C, et al. The diagnosis and management of thyroid nodules: a review. JAMA. 2018;319(9):914–24.
Deandrea M, et al. Determining an energy threshold for optimal volume reduction of benign thyroid nodules treated by radiofrequency ablation. Eur Radiol. 2021;31(7):5189–97.
Lee GM, et al. Successful radiofrequency ablation strategies for benign thyroid nodules. Endocrine. 2019;64(2):316–21.
Ebrahiminik H, et al. Radiofrequency ablation of benign thyroid nodules: initial clinical experience in Iran. Iran J Radiol. 2017;Special issue(5):e48418. https://doi.org/10.5812/iranjradiol.48418.
Bisceglia A, et al. Predictor analysis in radiofrequency ablation of benign thyroid nodules: a single center experience. Front Endocrinol. 2021;12:638880.
Kuo C-Y, et al. Learning curve analysis of radiofrequency ablation for benign thyroid nodules. Int J Hyperth. 2021;38(1):1536–40.
Nguyen VB, et al. Efficacy and safety of single-session radiofrequency ablation in treating Benign thyroid nodules: a short-term prospective cohort study. Int J Endocrinol. 2021;2021:7556393.
Kuo C-Y, et al. Computer-analyzed ultrasound predictors of the treatment efficacy of radiofrequency ablation for benign thyroid nodules. World J Surg. 2022;46(1):112–20.
Kim Y-S, et al. Radiofrequency ablation of benign cold thyroid nodules: initial clinical experience. Thyroid. 2006;16(4):361–7.
Feroci F, et al. Radiofrequency thermal ablation of benign thyroid nodules: the correlation between ultrasound nodule characteristics and results. Surgical Innovation. 2020;27(4):342–51.
Acknowledgements
The authors hereby would like to extend their gratitude to Dr. Hamid Moradi and Dr. Mehrzad Gholampour for their valuable comments.
Funding
The study did not receive any funding from external sources. It was conducted as part of the radiology residency thesis work without financial support from any institution or funding body.
Author information
Authors and Affiliations
Contributions
Z.M. and H.E. have designed the study. H.E. and H.C. have performed the RFA procedure on patients. All data collected and analyzed by Z.M. Also A.M., M.A.A and R.G had major role in the study supervision, Reviewing & Editing. Z.M. wrote the main manuscript text and all authors reviewed the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was conducted in compliance with all the principles of professional and scientific ethics along with the full observance of the confidentiality of patient information. Informed consent was further obtained from all participants. All experimental protocols were additionally approved by the Iran National Committee for Ethics in Biomedical Research with the code no. IR.AJAUMS.REC.1400.071, ensuring adherence to the guidelines set forth by this committee. Furthermore, the study followed relevant international clinical practice guidelines for radiofrequency ablation of benign thyroid nodules, to ensure the ethical conduct of the research and protection of human subjects.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Motaghed, Z., Chegeni, H., Mosadeghkhah, A. et al. Effect of ultrasound parameters of benign thyroid nodules on radiofrequency ablation efficacy. BMC Med Imaging 23, 85 (2023). https://doi.org/10.1186/s12880-023-01044-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-023-01044-z