- Research
- Open access
- Published:
Diagnostic value of combined CT lymphangiography and 99Tcm-DX lymphoscintigraphy in primary chylopericardium
BMC Medical Imaging volume 24, Article number: 223 (2024)
Abstract
Objective
To investigate the diagnostic value of combined 99Tcm-DX lymphoscintigraphy and CT lymphangiography (CTL) in primary chylopericardium.
Methods
Fifty-five patients diagnosed with primary chylopericardium clinically were retrospectively analyzed. 99Tcm-DX lymphoscintigraphy and CTL were performed in all patients. Primary chylopericardium was classified into three types, according to the 99Tcm-DX lymphoscintigraphy results. The evaluation indexes of CTL include: (1) abnormal contrast distribution in the neck, (2) abnormal contrast distribution in the chest, (3) dilated thoracic duct was defined as when the widest diameter of thoracic duct was > 3 mm, (4) abnormal contrast distribution in abdominal. CTL characteristics were analyzed between different groups, and P < 0.05 was considered a statistically significant difference.
Results
Primary chylopericardium showed 12 patients with type I, 14 patients with type II, and 22 patients with type III. The incidence of abnormal contrast distribution in the posterior mediastinum was greater in type I than type III (P = 0.003). The incidence of abnormal contrast distribution in the pericardial and aortopulmonary windows, type I was greater than type III (P = 0.008). And the incidence of abnormal distribution of contrast agent in the bilateral cervical or subclavian region was greater in type II than type III (P = 0.002).
Conclusion
The combined application of the 99Tcm-DX lymphoscintigraphy and CTL is of great value for the localized and qualitative diagnosis of primary chylopericardium and explore the pathogenesis of lesions.
Background
The incidence of primary chylopericardium is extremely low and was first reported by Hasebrock in 1888 [1]. The etiology and pathogenesis of this disease remain poorly understood. The pathological basis is that a variety of diseases that cause compression, obstruction, or rupture of the thoracic duct and lymphatic trunks (particularly the bronchomediastinal trunks) and can lead chyle into the pericardium [2]. Common disorders include congenital malformations of lymphatic vessels, ruptured lymphatic vessel injury, lymphatic vessel infiltration and obstruction by compression, subclavian vein embolism, and idiopathic chylopericardium [3]. Primary chylopericardium is characterized by the idiopathic accumulation of chylous fluid with a high concentration of triglycerides within the pericardial cavity, first proposed by Grove and Effler in 1954 [4]. Most patients with primary chylopericardium are asymptomatic at presentation. However, chest pressure, chest pain and shortness of breath have been reported. Patients are noted to have enlargement of the cardiac silhouette on routine Chest X-ray, and evidence of a pericardial effusion on echocardiography. The diagnosis is confirmed with pericardiocentesis and fluid analysis. The fluid is typically turbid white or milky in appearance, with a triglyceride level more than 500 mg/dL. Diagnostic imaging methods for this disease include direct lymphangiography (DLG), lymphoscintigraphy, CT lymphangiography (CTL), chest radiography, echocardiography, CT and MRI [5]. There have been fewer studies on the imaging manifestations of the disease, mostly case reports and small case studies. The purpose of this study was to use 99Tcm-DX lymphoscintigraphy to typify the manifestations of primary chylopericardium and to analyze the differences in CTL imaging manifestations between different 99Tcm-DX lymphoscintigraphy types. To investigate the diagnostic value of the combination of two imaging methods in the diagnosis of primary chylopericardium.
Information and methods
General information
Fifty-five patients of primary chylopericardium diagnosed from January 2016 to December 2021 in Beijing shijitan hospital were retrospectively analyzed. Inclusion criteria: (1) identified by physical exam or imaging studies, (2) all patients underwent pericardiocentesis and laboratory tests: ① milky white, yellowish celiac, reddish celiac, bloody celiac, etc. ② triglyceride > 1.25 mmol/L, ③ total cholesterol/triglyceride < 1, ④ mononuclear cells predominate, bacterial culture is negative, tuberculin test is negative, and there are no tumor cells, 1 point for each, and the diagnosis of chylopericardium can be confirmed with ≥ 2 points [6]. (3) all patients performed with 99Tcm-DX lymphoscintigraphy and CT lymphangiography (CTL). Exclusion criteria: (1) diseases that could lead to secondary chylopericardium such as malignancy, tuberculosis, infection, trauma, and subclavian vein thrombosis. (2) incomplete clinical or imaging data. A total of 89 patients with chylopericardium were included during the period, 12 were excluded due to secondary causes (including 8 cases of pericardial tuberculosis, 3 inflammatory cases, and 1 thoracic malignancy), and 22 were excluded due to incomplete clinical or imaging data, leaving 55 cases for final analysis(Fig. 1). Among these patients, 27 were males and 28 were females, aged between 2 and 72 years, with a median age of 25.75 years. The duration of the disease ranged from 20 d to 38 years. The first clinical manifestations included cough in 13 cases, cough with sputum in 4 cases, chest tightness and panic in 15 cases, shortness of breath in 9 cases, and asymptomatic in 17 cases. There were combined chylothorax in 18 cases, chylous ascites in 3 cases, chylous sputum in 2 cases, chyluria in 1 case, lymphedema of the upper limbs and face in 2 cases, and lower limb lymphedema in 1 case, with 10 cases of lymphatic malformation. The appearance of the chylous pericardial effusion was milky in 29 cases, pink in 10 cases, bloody in 6 cases, and yellow in 8 cases.
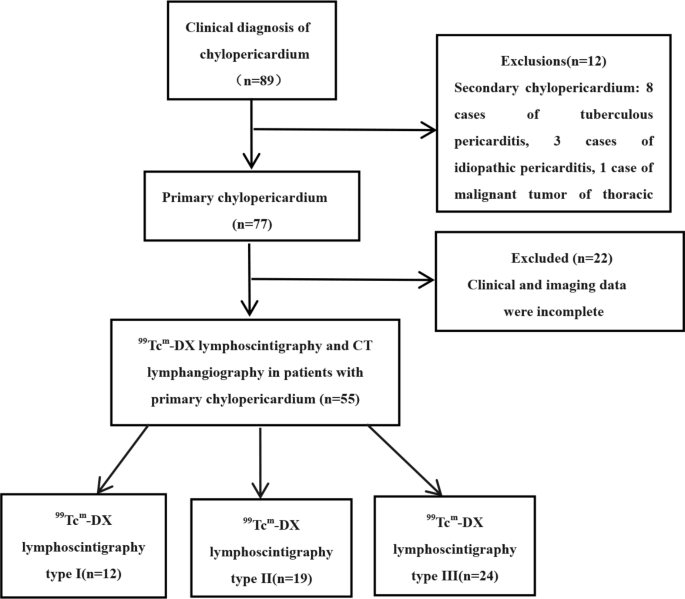
Flow chart of study population inclusion, 89 patients with chylopericardium were included between January 2016 and December 2021, 34 were excluded and finally 55 were included in the study
Imaging methods
All 55 patients underwent imaging studies utilizing 99Tcm-DX lymphoscintigraphy followed by spiral CT of the thoracic and abdominal CT regions. Patients were fasted and dehydrated before the CT examination.
99Tcm-DX lymphoscintigraphy was performed using the Siemens Symbia T16 dual-head SPECT system equipped with a low-energy high-resolution collimator. The peak energy was set to 140 keV, a window width of 20%, an acquisition matrix of 512 × 512. The images were acquired at a magnification of 1.0 and a speed of 14–18 cm/min. 99Tcm-DX was slowly injected subcutaneously into the first, second, and fourth, and fifth interphalangeal toes of both feet, with 111–185 MBq (0.10–0.15 ml) injected at each point. 99Tcm-DX was slowly injected subcutaneously between the 1st, 2nd, and 4th and 5th toes of both feet, with 111∼185 MBq (0.10∼0.15 ml) injected at each point. The volume and dose of injection were the same for both sides of the same patient, and the interval between injections was < 1 min. After 5 min of injection, patients were asked to walk on the ground, and those who could not walk were asked to do lower limb stretching exercises. Anterior and posterior whole-body imaging from foot to head was performed 10 min, 1 h, 3 h and 6 h after injection.
CTL was performed by direct lymphangiography (DLG) followed by DLG operation by a lymphatic surgeon. A mixture of 2% methylene blue and lidocaine (approximately 2 ml) was injected subcutaneously between the toes of a foot. Under microscopic guidance, a shallow lymphatic vessel stained with methylene blue was identified through an incision on the dorsum of the foot. Successful cannulation was followed by the infusion of iodized oil at a rate of 6–8 ml/h, with a total volume not exceeding 20 ml. Dynamic observation of the contrast agent’s flow through the lymphatic vessels, trunks, thoracic duct, and the thoracic duct’s termination into the bloodstream was monitored using DSA, with selective imaging performed for up to 4 h. CT scans of the chest and abdomen were performed 20 min to 2 h after the completion of DLG, using Siemens Sensation 16, Philips Brilliance iCT, and GE Revolution CT scanners. The scanning parameters included a tube voltage of 80–120 kV, tube current of 100–120 mA, slice thickness of 5–8 mm, interslice gap of 5–8 mm, reconstructed slice thickness of 2 mm, interslice interval of 1.8 mm, pitch of 1, and the scanning range extended from the inferior border of the thyroid cartilage to the inferior border of the pubic symphysis. The original axial MCST images were transferred to a workstation for multiplanar reconstruction (MPR), maximum intensity projection (MIP), and volume rendering (VR) post-processing to observe lymphatic vessels and other chest and abdominal CT.
Image analysis
Imaging analysis was conducted by two senior nuclear medicine physicians and two senior radiologists with over 10 years of experience(W Z, MX Z and YM Z, MK L), unawareness of clinical outcomes. Two senior physicians and radiologists analyzing the images reached a consensus on all cases or if there were any disagreements requiring further discussion. The 99Tcm-DX lymphoscintigraphy evaluation included: (1) the presence of abnormal radionuclide distribution at the jugular venous angle and the imaging status of the contralateral lymphatic vessels, (2) Whether the pericardium has an area of radioactivity defect and whether the delayed-imaging radioactivity is filled. Primary chylopericardium was classified into three types according to the presentation in 99Tcm-DX lymphoscintigraphy. Type I is abnormally concentrated, showing abnormal radioactive concentration of contrast agent in the left jugular vein angle. Type II is ectopic drainage, showing persistent concentration of contrast agent in the right jugular vein angle area, with or without radioactive concentration in the left jugular vein angle. And type III is an undemonstrative or transiently demonstrable type, which is characterized by undemonstrative left jugular vein angle or transiently demonstrable during the examination. 99Tcm-DX lymphoscintigraphy of the pericardium showed areas of radioactivity defects and delayed imaging of radioactivity filling suggestive of chylopericardium.
Abnormal distribution of contrast can indicate abnormalities in the lymphatic vascular system. Abnormal CTL primarily manifested as multifocal abnormal distribution of the contrast agent, appearing tubular, mass-like, clustered, or irregularly distributed, either continuously or discontinuously within and outside the lymphatic circulation. Abnormal contrast distribution in the ipsilateral iliac group and lumbar trunk referred to increased contrast presence in the imaging side’s iliac group and lumbar trunk. Lymphatic reflux was defined as the presence of contrast agent on the contralateral side of the imaging side, such as in the contralateral lumbar trunk, presacral region, iliac fossa, cervical trunk, and subclavian trunk, indicative of lymphatic reflux. CTL imaging analysis included: (1) abnormal contrast distribution and reflux in the neck, subclavian area, end of the thoracic duct, end of the right lymphatic duct and axilla, (2) abnormal contrast distribution in the chest, including deep thoracic areas (anterior mediastinum, main pulmonary artery window, trachea and bronchial surroundings, sub-carina, posterior mediastinum, hilum, peribronchovascular bundle, and pericardium) and superficial thoracic areas (intercostal, pleural, and above the diaphragm), (3) thoracic duct dilation was defined as the widest diameter of the thoracic duct > 3 mm [7], (4) Abnormal contrast distribution of subdiaphragmatic, ipsilateral iliac group, lumbar trunk, contralateral iliac group, contralateral lumbar trunk reflux, and abnormal contrast distribution of retroperitoneal .
Statistical analysis
Statistical analysis was conducted using SPSS 26.0. Normally distributed quantitative data were expressed as mean ± standard deviation, while non-normally distributed data were expressed as median ± interquartile range. For quantitative variables, if they were normally distributed and homogeneity of variance was satisfied, independent sample T-tests and one-way ANOVA were used to detect inter-group differences. Otherwise, the Mann-Whitney test or Kruskal-Wallis H test was employed. For categorical variables, the chi-square test was used to detect inter-group differences. P-value < 0.05 was considered statistically significant.
Results
99Tcm-DX Lymphoscintigraphy
The 99Tcm-DX lymphoscintigraphy categorized 12 cases as Type I (Fig. 2A), 19 cases as Type II (Fig. 3A), and 24 cases as Type III (Fig. 4A). Forty cases of 99Tcm-DX lymphoscintigraphy suggestive of chylopericardium (40/55, 72.7%).

A99Tcm-DX lymphoscintigraphy type I, abnormal radioactive concentration in the left jugular corner (black arrow). B CTL showed abnormal contrast distribution in the left jugular corner, retroperitoneal and iliac groups (black arrow)

A99Tcm-DX lymphoscintigraphy type II, abnormal radioactive concentration in the right jugular corner area, accompanied by radioactive concentration in the left jugular corner. B CTL showed abnormal contrast distribution at the end of the thoracic duct, posterior mediastinum, and right iliac group ( arrowhead)

A99Tcm-DX lymphoscintigraphy type III, left jugular horn was not developed or was temporarily developed during the examination. B CTL showed abnormal contrast distribution in the peribronchial, lower bulge, left iliac group, and retroperitoneum (The black arrow)
CT Lymphangiography (CTL)
The incidence of abnormal contrast distribution in the bilateral cervical or subclavian areas was significantly higher in Type II of 99Tcm-DX lymphoscintigraphy than in Types I and III (P = 0.000), indicating a statistically significant difference. The rate of abnormal contrast distribution in the main pulmonary artery window was significantly higher in Type I compared to Type III (P = 0.009). Similarly, the rate of abnormal contrast distribution adjacent to the pericardium was significantly higher in Type I compared to Type III (P = 0.002), predominantly on the left side. The occurrence of abnormal contrast distribution around the trachea and bronchi was significantly higher in Type II compared to Type III (P = 0.001). A statistically significant difference was also observed in the rate of abnormal contrast distribution in the posterior mediastinum (P = 0.001) (Fig. 2B、3B、4B, Table 1).
Discussion
The normal pericardial cavity usually contains 25‑35 ml of fluid, and the cardiac lymph vessels drain the pericardial fluid to the left subclavicular vein via the mediastinal lymph vessels, lymph nodes, and thoracic ducts [8]. Chylopericardium can be categorized into primary and secondary chylopericardium characterized by the accumulation of triglyceride-rich celiac effusion within the pericardial cavity. The incidence of primary chylopericardium was 56% [3]. Primary chylopericardium can only be diagnosed when there is a secondary etiology such as cardiothoracic surgery, trauma, radiotherapy, infection, tuberculosis, cervical mediastinal lymphangioma, multiple osseous lymphangiomas, lymphomas, and other malignant tumors, venous obstruction, and acute necrotizing pancreatitis [9,10,11]. The etiology and pathogenesis of primary chylopericardium remain unclear. Akamatsu et al. [12]. suggested that it was related to (1) functional impairment of the branch valves with abnormal transportation of the thoracic duct and pericardial lymphatics, (2) increased pressure in the thoracic duct caused by lymphatic dilatation, (3) the presence of an abnormal transportation between the lymphatic duct and the pericardial cavity. Chylopericardium due to lymphatic malformation is rare. The disease is mainly seen in young adults, with no gender difference. The progression of the disease is slow, and some patients are asymptomatic for several years or more than ten years, and the enlargement of the heart is often found on chest X-ray during physical examination [13]. Common initial symptoms include dyspnea and cough, with other manifestations such as palpitations, chest pain, gastrointestinal symptoms, syncope, fatigue, and edema [14, 15]. A small number of patients with chronic pericardial effusion may develop cardiac tamponade due to obstructed venous return and reduced cardiac output. Physical examination often reveals typical signs of pericardial effusion such as enlarged cardiac silhouette, distant heart sounds, and paradoxical pulse, with prolonged disease course leading to enlarged liver and spleen, distended neck veins, ascites, and edema. There are no definitive diagnostic criteria for this condition, but it can be qualitatively diagnosed based on clinical presentation, echocardiographic findings, the appearance of pericardial fluid, positive Rivalta test, and chylomicron presence. We summarize previous studies and propose diagnostic criteria [3, 5]: (1) milky white, pale yellow chylous, pale red chylous, hemorrhagic chylous, and coffee-colored appearance, (2) triglycerides > 1.25 mmol/L or pericardial effusion triglyceride levels exceeding simultaneous blood levels with lower total cholesterol, total protein, and albumin levels compared to blood, (3) cholesterol/triglyceride ratio < 1, (4) negative bacterial culture or predominantly mononuclear cells with a monocyte ratio > 85%. One point for each feature, greater than 2 points for a diagnosis of chylopericardium.
Chest X-ray, echocardiography, CT and MRI are important tools in primary chylopericardium. Chest X-ray may show an enlarged cardiac shadow, and echocardiography may clarify the amount and location of pericardial effusion and localize the puncture. CT and MRI imaging can help to clarify the relationship of the thoracic duct to pericardial effusion. Radionuclide lymphoscintigraphy and CTL are also effective diagnostic tools [16]. Radionuclide lymphoscintigraphy using 99Tcm-labeled human albumin can identify the location of pericardial effusion, assess cardiac size and shape, and differentiate between pericardial effusion, cardiac enlargement, and cysts. Both radionuclide lymphoscintigraphy and CTL can determine the presence of lymphatic reflux and abnormalities around the pericardium, mediastinum, and thoracic duct, and accurately diagnose the etiology of chylous pericardial effusion. 99Tcm-DX lymphoscintigraphy is a non-invasive method for the diagnosis of this disease and can dynamically display lymphatic reflux [17].
All the cases in our study were categorized into 3 types based on the abnormal presentation of 99Tcm-DX lymphoscintigraphy: Type I (abnormal concentration), Type II (ectopic drainage), and Type III (non-imaging or transient imaging). Abnormal tracer concentration in Types I and II may be related to: (1) thoracic duct terminal obstruction causing lymphatic reflux obstruction (2) increased jugular venous angle backflow pressure leading to chyle outflow obstruction (3) Lymphatic fluid production is excessive, chylous fluid into the blood mouth is relatively narrow. 99Tcm-DX lymphoscintigraphy type II showed continuous development of bilateral venous angles, suggesting malformation of the thoracic duct and the possibility of double venous angular drainage with outlet obstruction. Type III, characterized by no imaging or transient imaging at the left jugular venous angle during the examination, may be due to low resolution of 99Tcm-DX lymphoscintigraphy or tracer retention in the lower limbs or leakage into the thoracoabdominal cavity, preventing reach to the thoracic duct terminal. 99Tcm-DX lymphoscintigraphy is clinically significant for identifying chylopericardium, chylothorax, and chyloperitoneum caused by thoracic duct obstruction, though it has lower resolution and less accuracy in detailing lesions compared to CTL. The high-density resolution of CTL not only reveals abnormalities of the thoracic duct and its branches, but also clearly shows abnormalities of the surrounding tissue structures, such as the degree and extent of pericardial effusion.
The results showed that the combined application of 99Tcm-DX lymphoscintigraphy and CTL is of great significance in the diagnosis of the location, extent and degree of systemic lymphatic abnormality in primary chylopericardium. The incidence of abnormal contrast distribution in the cervical or subclavian areas showed statistically significant differences among the different types of 99Tcm-DX lymphoscintigraphy (P = 0.000). A two-by-two comparison revealed a statistically significant difference in the distribution of contrast abnormalities in the bicervical or subclavian region, which was greater in type II than in types I and III (P = 0.000). The study demonstrated the significant diagnostic value of combining 99Tcm-DX lymphoscintigraphy with CT lymphangiography (CTL) for identifying the location, extent, and severity of primary chylopericardium and its related lymphatic anomalies. The incidence of abnormal contrast distribution in the bilateral cervical or subclavian regions showed significant differences among the groups in the 99Tcm-DX lymphoscintigraphy (P = 0.000), with Type II exhibiting a greater incidence than Types I and III. 99Tcm-DX lymphoscintigraphy type II suggests the presence of a double thoracic duct or right-sided thoracic duct malformation, with an abnormal distribution of contrast in the double cervical or subclavian region suggesting concomitant right cervical and subclavian lymphatic reflux, and the thoracic duct may be double stemmed or right-sided thoracic duct variant, which is consistent with the 99Tcm-DX lymphoscintigraphy. This study found that 34.5% of primary chylopericardium were associated with double or right-sided thoracic duct variations. There was also a correlation between 99Tcm-DX and CTL findings, with statistically significant difference in the distribution of contrast in the posterior mediastinum, suggesting that this might relate to abnormal reflux, dilation, or constriction of the thoracic duct. Abnormal contrast distributions around the pericardium and the main pulmonary artery window were more prevalent in Type I compared to Type III (P = 0.009 and P = 0.011, respectively), indicating that obstruction at the terminal part of the thoracic duct and associated lymphatic abnormalities near the pericardium and the main pulmonary artery window might play a role in the pathogenesis of primary chylopericardium. CTL was instrumental in visualizing the location and distribution of abnormal lymphatic vessels, contributing to the understanding of the disease mechanism and imaging characteristics of lymphatic anomalies in primary chylopericardium.
Conservative management is tried initially in most patients diagnosed with primary chylopericardium. However, in some cases the treatment of chylopericardium may be surgical. When the course of the thoracic duct was identified exactly, ligation and resection of the thoracic duct with establishment of a pericardial window proved to be the most effective surgical procedure. The combination of 99Tcm-DX lymphoscintigraphy and CTL is instructive in the preoperative management of primary chylopericardium due to abnormal thoracic duct pathways.
There are limitations of this study: (1) This study is retrospective and has a small sample size. (2) This study did not include other methods of imaging examination, such as DLG and MRI, etc. The next study can include DLG and MRI examination methods for comprehensive analysis.
In summary, 99Tcm-DX lymphoscintigraphy is non-invasive, simple and repeatable imaging method. CTL can clearly show the location, degree and surrounding tissue of systemic lymphatic vessel abnormality. The combined application of the two methods is of great value for the diagnosis and pathogenesis of primary chylopericardium.
Data availability
Data is provided within the supplementary information files.
Abbreviations
- CTL:
-
CT lymphangiography
- DLG:
-
Direct lymphangiography
References
Hasebrock K. Analyse Einer Chylosen Pericardierlen Flussigkeit (chylopericardium). Ztschr Physiol Chemie. 1888;12:289.
Kwon JB, Choi SY, Kim CK, Park CB. Primary idiopathic silent chylopericardium. J Cardiothorac Surg. 2013;8:28.
Dib C, Tajik AJ, Park S, et al. Chylopericardium in adults: a literature review over the past decade (1996–2006)[J]. J Thorac Cardiovasc Surg. 2008;136(3):650–6.
GROVES L K. EFFLER D B. Primary chylopericardium[J]. N Engl J Med. 1954;250(12):520–3.
Cellina M, Martinenghi C, Panzeri M, Soresina M, Menozzi A, Daniele G, Oliva G. Noncontrast MR Lymphography in secondary Lower Limb Lymphedema. J Magn Reson Imaging. 2021;53(2):458–66.
Staats BA, Ellefson RD, Budahn LL, et al. The lipoprotein profile of chylous and nonchylous pleural effusions[J]. Mayo Clin Proc. 1980;55(11):700–4.
Kiyonaga M, Mori H, Matsumoto S, et al. Thoracic duct and cisterna chyli: evaluation with multidetector row CT[J]. Br J Radiol. 2012;85(1016):1052–8.
Yu X, Jia N, Ye S, et al. Primary chylopericardium: a case report and literature review[J]. Exp Ther Med. 2018;15(1):419–25.
Raza M, Matar K. Idiopathic chylothorax and chylopericardium resistant to conservative and surgical management[J]. Heart Lung Circ. 2009;18(3):229–32.
Courtney M, Ayyagari RR. Idiopathic chylopericardium treated by percutaneousthoracic duct embolization after failed surgical thoracic duct ligation[J]. Pediatr Radiol. 2015;45(6):927–30.
Ossiani MH, McCauley RG, Patel HT. Primary idiopathic chylopericardium[J]. Pediatr Radiol. 2003;33(5):357–9.
Akamatsu H, Amano J, Sakamoto T, et al. Primary chylopericardium[J]. Ann Thorac Surg. 1994;58(1):262–6.
Mallon NG, Nmke L, McCann et al. Isolated chylopericardium.Surgeon, 2003, l: 236.238.
Kwon JB, Choi SY, Kim CK, Park CB. Primary idiopathic silent chylopericardium. J Cardiothorac Surg. 2013;8(1):28.
Han Z, Li S, Jing H, Liu H. Primary idiopathic chylopericardium: a retrospective case series. BMC Surg. 2015;15(1):61.
Itkin M, Swe NM, Shapiro SE, Shrager JB. Spontaneous chylopericardium: delineation of the underlying anatomic pathology by CT lymphangiography. Ann Thorac Surg. 2009;87(5):1595–7.
Chen FC, Huang JL, Lin WY, Ting CT. Pedal Tc-99m phytate lymphoscintigraphy in primary chylopericardium. Int J Cardiol. 2003;90(2–3):341–3.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (61876216) and Beijing Municipal Commission of Science and Technology (Z211100003521009).
Funding
This work was supported by the National Natural Science Foundation of China (61876216) and Beijing Municipal Commission of Science and Technology (Z211100003521009).
Author information
Authors and Affiliations
Contributions
(I) Conception and design: YM Zhang, RG Wang; (II) Administrative support: XP Li; (III) Provision of study materials or patients: MK Liu; (IV) Collection and assembly of data: YM Zhang; (V) Data analysis and interpretation: MX Zhang; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by institutional ethics board of beijing shijitan hospital (IIT2024-059-001) and individual informed consent for this retrospective analysis was waived.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Y., Wen, Z., Liu, M. et al. Diagnostic value of combined CT lymphangiography and 99Tcm-DX lymphoscintigraphy in primary chylopericardium. BMC Med Imaging 24, 223 (2024). https://doi.org/10.1186/s12880-024-01399-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12880-024-01399-x